
The other day, I was perusing the hellsite known as Twitter before it becomes even more of a hellsite after Elon Musk acquires it, when I came across this series of Tweets about a favorite topic of this blog for the last year and a half, the Great Barrington Declaration. I’ll quote the first few, so that you can see why they would have interested me, namely because they are about a study that provides yet more evidence to support what I’ve been arguing about the Great Barrington Declaration ever since it was first published:
Even though I’ve decreased my blogging frequency because my wife and I are fostering puppies again, I knew I had to write about this study. First, however, let’s take a look at the puppies.

Then, let’s briefly review what the Great Barrington Declaration is and what its effects have been before moving on to the study itself.
The Great Barrington Declaration: Propaganda, not science
I’ve written a number of times about the Great Barrington Declaration, a document written by three “lockdown” hating scientists recruited for a meet-and-greet with sympathetic journalists at the headquarters of the American Institute for Economic Research (AIER), a right wing “free market” think tank in Great Barrington, MA, the town that gave the declaration its name. The basic idea behind the Great Barrington Declaration, which was published in early October 2020, was that “lockdowns” were doing more harm than COVID-19. Based on this premise, the authors (Profs. Martin Kulldorff, then faculty at Harvard University, Jay Bhattacharya of Stanford University, and Sunetra Gupta of Oxford University) proposed, in essence, a “let ‘er rip” strategy for COVID-19 in order to reach “natural herd immunity” more rapidly by infecting those least likely to die from the disease. The idea was to lift protections and let the young and “healthy” go back to “normal life,” while using “focused protection” to keep the elderly and those with chronic health conditions who were at much higher risk for severe disease and death from contracting COVID-19.
As I originally wrote the very first time I discussed the Great Barrington Declaration, the idea of “focused protection” was long on claimed benefits but very short on policy specifics regarding how, exactly, those vulnerable to the worst outcomes from COVID-19 infection would be “protected” while ignoring that, even among the “low risk” population, a “let ‘er rip” policy like that espoused by the Great Barrington Declaration authors would still result in mass death and morbidity. Indeed, a number of respected public health scientists responded with the John Snow Memorandum, which argued that mass infection was not a viable strategy and explained why “let ‘er rip” would be far more harmful than letting the young develop “natural immunity” (more appropriately referred to as postinfection immunity) in a strategy to speed the achievement of “natural herd immunity.” (For a detailed explanation why the Great Barrington Declaration couldn’t have worked, I recommend this article, as well as an BMJ Rapid Response written by a Local Councillor in the UK who described in detail the practicalities that would have made a “focused protection” strategy almost certain to fail.
The Great Barrington Declaration was what I referred to as “magnified minority”; i.e., a document written by fringe physicians and/or scientists and then signed by a lot of other physicians and/or scientists in order to give the impression that the statements in the document are scientifically worthy of consideration. For purposes of the propaganda value of such a document, it doesn’t matter one whit if the signatories have the relevant expertise or not; all that matters is that they have advanced degrees after their names, in order to give the appearance to the public that a large number of experts endorse the document. Moreover, “magnified minority” is a common tactic by science deniers and has been used by, for example, cranks who claim that HIV doesn’t cause AIDS, climate science deniers, and evolutionists. (Does anyone remember Scientific Dissent from Darwinism?)
The Great Barrington Declaration was the same tactic. It was also profoundly eugenicist, as I argued right from the start, in that it left the elderly and those with chronic illnesses to the tender mercies of SARS-CoV-2 while only paying lip service to actually protecting them. This was especially true in October 2020, a time when it was generally thought that a safe and effective vaccine against COVID-19 wouldn’t be available for at least a few more months. Even though the Pfizer vaccine did roll out two months later in December, quantities were very limited at first, with availability limited to healthcare and other frontline workers until well into early 2021.
Unfortunately, Great Barrington Declaration supporters, despite their constant claims of “persecution” and being “silenced,” basically won the PR and policy battle. In 2020, its authors easily gained access to the highest levels of government in the US and Europe to argue against “lockdowns,” and Jeffrey Tucker left the AIER to spawn another right wing think tank, the Brownstone Institute, which he lovingly characterized as the “spiritual child” of the Great Barrington Declaration and for which he recruited Martin Kulldorff as scientific director. AIER, Brownstone Institute, and a host of other “free market” anti-regulation astroturf rapidly became the new merchants of doubt about public health and struck back at critics who pointed out the connections between right wing think tanks and anti-public health activities increasingly linked to the far right and its media ecosystem.
Even worse, increasingly the Brownstone Institute and others promoting the Great Barrington Declaration are spreading misinformation that is more and more explicitly antivaccine and attacking vaccine advocates on social media while portraying vaccine and mask mandates, as well as “lockdowns,” as slavery, religion, fascism, and Communism, apparently depending on what day of the week it is. You’d think that there is no greater tool for a “focused protection” strategy than a safe and effective vaccine against COVID-19 and that Great Barrington Declaration authors and advocates would want to encourage vaccination of as many people as possible. You’d be mistaken. At least two of the authors, plus the founder of the Brownstone Institute, have openly embraced fantasies of retribution against public health advocates very much like the sorts of fantasies of retribution antivaxxers have held for decades, in particular the idea of a “Nuremberg 2.0,” a Nuremberg-style tribunal in which public health advocates will “be held accountable” for their supposed “crimes.”
Of course, it’s obvious in retrospect that a “natural herd immunity strategy would never have worked. One has only to cite the rise of the Delta and the Omicron variants, the latter of which has been able to overcome vaccine-induced immunity in many people but postinfection immunity as well. Even without the rise of these variants, an entirely predictable event when a virus circulates in a large enough immunologically naive population for long enough, no disease has ever been controlled solely through “natural herd immunity.” Other measures, especially vaccines, are necessary. Worse, even if COVID-19 could have been controlled through a “natural herd immunity” approach, the death toll would have been even more horrific than it already has been, given that the US alone has suffered close to a million fatalities (almost certainly a gross underestimate), and the world many times that.
Which brings us back to the study, Critical weaknesses in shielding strategies for COVID-19, published by Smith et al in PLoS Global Public Health a couple of days ago. Kit Yates, whose Tweets I quoted, is a coauthor.
“Focused protection” wouldn’t have worked
This paper was written by a group from the University of Bath in the UK consisting of Cameron Smith, Christian Yates, and Ben Ashby. The first thing you need to know is that they’re all in the Department of Mathematical Sciences and that this is a modeling paper. Another interesting thing, looking at the metrics of the article, is that the study, although covered fairly widely in the press, didn’t achieve nearly the coverage in the press or social media that a number of highly dubious papers that amplified COVID-19 contrarian takes on the pandemic. (Just compare the metrics for John Ioannidis’ math-challenged “science Kardashians” article or Paul Thacker’s “Pfizer whistleblower” conspiracy theory article months after their publication if you don’t believe me.)
The other interesting thing is that the model, based on real world data, appears to support what I’ve always intuitively thought about the Great Barrington Declaration, namely that it would require perfection to have even a hope that “focused protection” would work. After all, the elderly and many with comorbidities who are at the highest risk of hospitalization and death from COVID-19 require care (or at least help) from the young and “healthy” population in which “natural herd immunity” is being sought. Think about it. All it takes is one infection in a nursing home to start an outbreak that could kill many of its frail residents. We’ve seen it. The same is true for any multigenerational house in which elderly or chronically ill people live with younger “healthy” family members who provide some level of care to them. How do you keep the contact between, say, a parent with early stage Alzheimer’s disease living with their adult child who cares from them, to zero? You can’t; that is, unless one or the other moves out.
In their introduction, the authors provide this rationale for their study:
Prior to (and during) the rollout of vaccines, most countries introduced a range of non-pharmaceutical interventions (NPIs) to bring infections under control, including social distancing, travel restrictions, and lockdowns. While the effectiveness of different NPIs has varied within and between populations and over time, they have been largely effective at bringing outbreaks under control [2–4]. A widely discussed alternative approach would have been to limit most NPIs to the most vulnerable subpopulations while allowing those at lower risk to live with few or no restrictions [4–6]. ‘Shielding’ (or ‘focused protection’), appeared to offer the possibility of avoiding the various societal costs of universal NPIs by leveraging the uneven risk profile of COVID-19, which is heavily skewed towards the elderly and those with certain pre-existing conditions [7, 8]. In theory, by allowing infections to spread with little to no suppression among the lower-risk population during a temporary shielding phase, the higher-risk population would subsequently be protected by herd immunity [9]. Several countries either openly or reportedly embraced this strategy during the early stages of the pandemic. Sweden, for example, chose to impose few restrictions on the general population while banning visits to long-term care (LTC) facilities [10], and the UK initially appeared to opt for a shielding strategy [11] before implementing a national lockdown. In the autumn of 2020, many countries experienced a resurgence in infections following the lifting of NPIs, leading to a renewed debate about the merits of shielding, driven by the Great Barrington Declaration which called for “focused protection of older people and other high-risk groups” while allowing uncontrolled viral transmission among lower-risk individuals [12, 13].
However, they also note:
It is important to retrospectively assess the feasibility of shielding as a public health strategy, not only for public inquiries into COVID-19 and future pandemic preparedness, but also for countries where levels of vaccination remain low. Moreover, new variants may emerge which substantially escape vaccine-induced immunity, thus requiring a renewed choice between lockdowns and shielding while vaccines are updated. Although superficially appealing, serious practical and ethical concerns have been raised about shielding as a strategy to mitigate the impact of COVID-19 [14]. Yet there has been little mathematical modelling to determine the effectiveness of shielding under realistic conditions [4–6]. Crucially, the combined consequences of imperfect shielding, uneven distributions of immunity, and changes in contact behaviour among lower-risk individuals have yet to be explored.
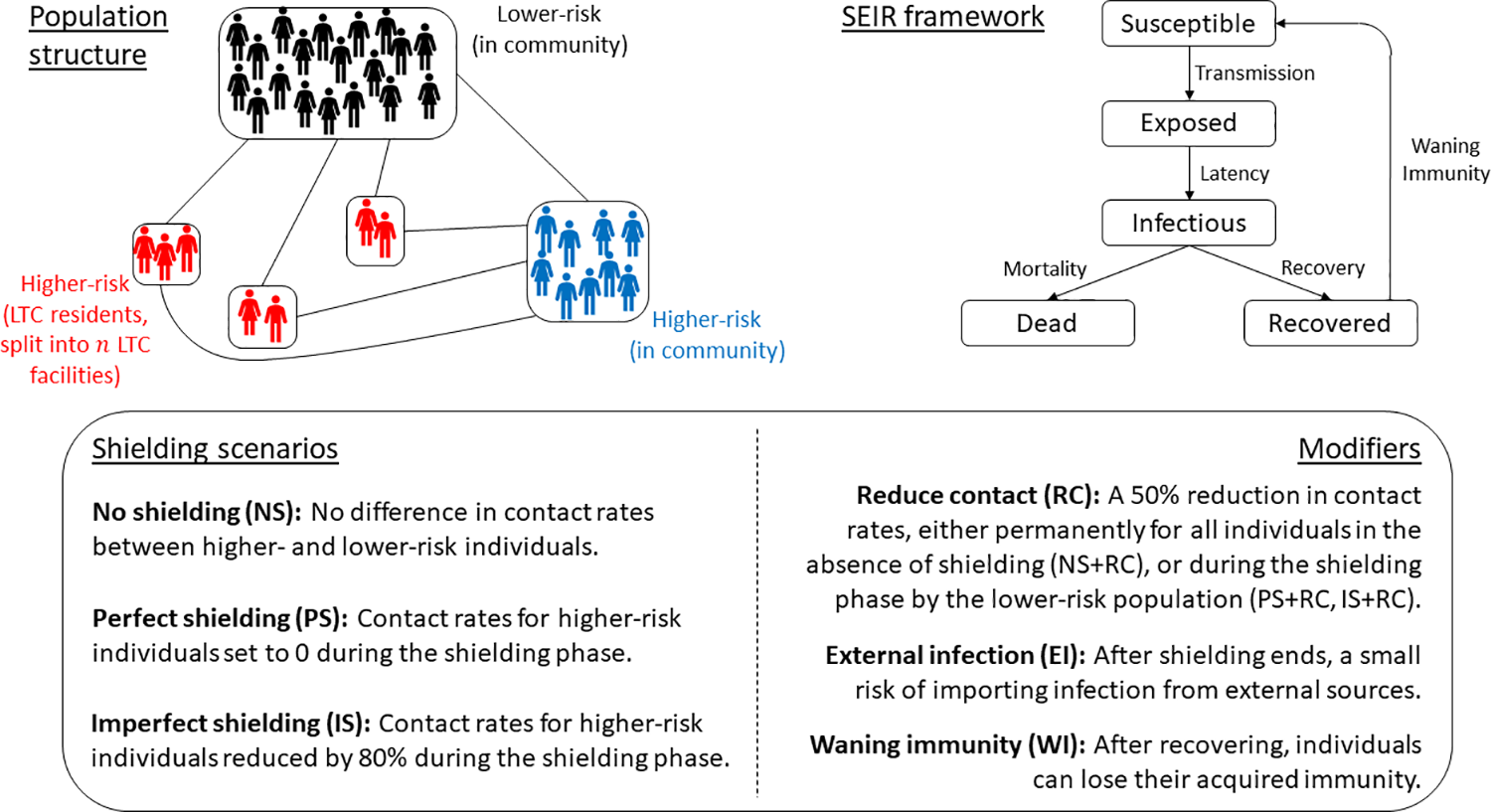
So explore them the authors did, using a model designed to simulate early stages of a pandemic, when the virus encounters an immunologically naïve population for the first time, with the following parameters and assumptions:
Our model is loosely based on an idealized large city in England (although our qualitative results would apply to similar countries) consisting of 1 million people, 7% of whom are at higher-risk of mortality from COVID-19, with 10% of higher-risk individuals situated in LTC facilities [15, 16]. We compare epidemics under no shielding, with imperfect (partial reduction in contacts for higher-risk individuals) and perfect shielding (no contacts for higher-risk individuals), with shielding restrictions lifted when cases fall below a given threshold (see §2.1).
To address the question of whether a Great Barrington Declaration-like “focused protection” strategy could have worked, the authors modeled a hypothetical large city in England with a population of one million, using an SEIR (Susceptible, Exposed, Infected, Removed) model. They compared the outcomes from no shielding, with imperfect and perfect shielding, with shielding restrictions lifted when cases fall below a given threshold. The framework for the model looks like this:
The mathematical analysis is quite complex, as you might imagine, and I’m sure there are mathematicians who could critique it much better than I. In any event, the first finding is that, in theory, it is possible that a Great Barrington Declaration-like “focused protection” approach could have worked to keep the most vulnerable from dying in droves. There are some serious problems, though. First, the protection would have had to have been perfect, with 0% contact between the “healthy” out there catching COVID-19 for the greater good of achieving “natural herd immunity” faster and those who, through either age or chronic health conditions, were at much higher risk of dying from the disease. Basically, the level of shielding would, as a practical matter, have been impossible to achieve, which means that infections from the lower-risk population would have inevitably leaked through “focused protection” to the vulnerable.The second problem is that, even assuming the most optimistic conditions, hospitals would have been completely overwhelmed—by at least ten-fold!—by the first wave of infections. In addition, even if the lower risk people out there catching COVID-19 to achieve “natural herd immunity” started reducing social contact to avoid infection, thus slowing the increase in case numbers and thereby taking some pressure off of the hospitals, the model suggests that it would likely have been impossible to achieve “natural herd immunity,” which would have made a second wave of infections after shielding ended almost inevitable. Moreover “natural immunity” would have been unevenly distributed in the population, which would have led to the risk of local outbreaks.
Or, as the authors put it:
Our results demonstrate critical epidemiological weaknesses in shielding strategies that aim to achieve herd immunity by isolating the vulnerable while allowing infections to spread among lower-risk members of the population. While our main results focus on a limited set of parameters, our findings are qualitatively robust to sensitivity analysis (§A of the S1 Text). Even in the best-case scenario with perfect shielding, our model estimates that there would have been tens of thousands of avoidable deaths among those deemed to be at lower risk due to limited mitigation in this subpopulation, even without accounting for the rapid depletion of healthcare capacity. A significant reduction in contact rates would have been required to avoid overwhelming healthcare capacity during shielding [18], but the population would have then failed to achieve herd immunity, allowing a second, deadlier wave to occur following the lifting of restrictions. Under more realistic assumptions of imperfect shielding, our model estimates that deaths would have been 150% to 300% higher compared to perfect shielding.
And also:
Our model demonstrates that shielding would have only worked well under practically unrealizable conditions. If any of these conditions had not been met, then significant outbreaks would have occurred in higher-risk subpopulations, leading to many more deaths than if shielding were perfect. To be effective, shielding would have also required those who were at higher risk to not only be rapidly and accurately identified, but also to shield themselves for an indefinite period. If higher-risk individuals were to be misdiagnosed or were unable to fully isolate this would have decreased the effectiveness of shielding. For example, shielding would have been especially difficult for households that contained both higher- and lower-risk individuals (e.g., 74% of CEV people in England live with other people, and 15% live with children aged under 16 years [29]). The large number of multi-risk households suggests that either shielding would have been far from perfect, or a significant proportion of lower-risk individuals would have also had to shield, in which case it would have been harder (or perhaps impossible) to achieve herd immunity during the shielding phase.
In practice, according to this model, the Great Barrington Declaration would have been a disaster.

It’s only a model, but it’s a best case scenario model
But, but, but, but… you say (and Great Barrington Declaration supporters retort), it’s only a model! Yes, it is. It’s a model. However, that doesn’t help Great Barrington Declaration fans, because this is actually a model that is based on some pretty optimistic assumptions. Indeed, the authors appear to have gone out of their way to use assumptions that were conservative, best case scenarios even.
As the authors note:
Our model also made conservative assumptions regarding infection fatality rates (IFRs; see §2.1) and immunity, but more realistic assumptions are likely to make the case for shielding far worse. For example, we used relatively low estimates for the IFRs and assumed that these were fixed even though healthcare capacity would have been significantly overwhelmed under all shielding scenarios. The model also did not capture the impact of healthcare burden on mortality from other causes.
Again, these are all very optimistic assumptions.
Even worse (for the Great Barrington Declaration, not the model), the authors note that the model did not take into account the potential evolution of SARS-CoV-2:
A large epidemic would have also potentially allowed new variants to emerge, which may have been more transmissible, more deadly, or able to escape immunity. We made the conservative assumption of no pathogen evolution, but novel variants would have rendered shielding an even less effective strategy.
We know that variants arose that fulfilled two out of those three criteria. The Delta and Omicron variants were not more deadly than the original strain, but they were more transmissible and—especially the Omicron variants—better at evading immunity. The Delta variant arose last summer and was much more transmissible than the original Wuhan strain. It was followed by the Omicron variants this winter, which were even more transmissible and able to evade prior immunity, leading to many more “breakthrough” infections after vaccination and to reinfections in those who had recovered from COVID-19.
It’s long been pointed out that the fatal flaw in the thinking (if you can call it that) behind the Great Barrington Declaration is that it never took into account what virologists knew even in October 2020 to be the high likelihood that new variants would arise that were more transmissible and possibly even able to evade immunity due to prior infection. (Again, remember that the Great Barrington Declaration was written months before vaccines started rolling out to the population in large quantities, and then primarily in developed nations.) This model assumes what Great Barrington Declaration signatories apparently actually believe, even though it’s not true:
We further assumed that immunity from infection was perfect and long-lasting (‘best-case’ assumptions for shielding), but neither is likely to be true in reality
We now know that immunity from infection was robust but nowhere near long lasting, as evidenced by the number of reinfections. As I’ve discussed before, “natural immunity” due to infection doesn’t appear to be much longer lasting than vaccine-induced immunity.
All of this is why the authors concluded:
These additional considerations, in combination with the clear flaws indicated by our modelling, suggest that, while an idealized shielding strategy may have allowed populations to achieve herd immunity with fewer deaths, they are likely to have failed catastrophically in practice.
A good rule of thumb is that a strategy that requires perfect execution in order to have a chance of working is a strategy that is not going to work.That describes the Great Barrington Declaration very well. Of course, the Great Barrington Declaration was never a serious strategy. It was propaganda with a veneer of science just convincing enough to sound reasonable to people without a lot of knowledge of infections disease, epidemiology, or public health, whose understanding of “herd immunity” is superficial, and its purpose was to provide a seemingly scientific rationale to do what right wing “free market” groups wanted to do anyway: Stop business closures and government public health restrictions and mandates. Stop collective action in the service of public health. Weaken the administrative state.
Unfortunately, the astroturf groups manipulating useful idiots like Martin Kulldorff into producing the Great Barrington Declaration succeeded wildly, no matter how much Kulldorff and his crew whine about being “silenced” and fantasize about retribution against public health advocates or AIER portrays itself as akin to persecuted abolitionists.
Of course, the Great Barrington Declaration was never a viable plan to deal with the pandemic. It was never intended to be and didn’t have to be. It was propaganda all along.

77 replies on “The Great Barrington Declaration never would have worked”
Hi. This is an extremely pedantic point and does not detract at all from the article or arguments. I’m the author of that BMJ rapid response.
The role of a Local Councillor in the UK is a little murky, but is not really that of a Government Official. It’s a volunteer role to which you have win election, undertaken in addition to any full-time job.
In normal life, we act to represent our residents to the Council and the Council to our residents; a line of communications and representation in both direction. In addition, we work with the Local Authority officers/officials (who do have this as a full-time job – and are prohibited for standing for election to Council) to ensure these views and representations are taken into account in both directions. Further to that, we act to scrutinise Council actions and, if the dominant party, lay down policy and direction overall to which the officers work.
It’s made more complicated in times of emergency, as the Local Authorities plug in to something called the Local Resilience Forum, nationwide, where Councils are effectively co-opted into the national response – both to bring in information at the local level and act as the last-mile deliverers on many things. As it happens, our Council’s CEO (the seniormost officer; not a Councillor) was brought into the Gold Command level of the LRF, sitting immediately under COBRA.
(So, arguably, he did effectively become a government official rather than a Council official at that point).
The shielding, community support, and vaccine rollout were all delegated through the LRF structure to the Local Authorities (various Councils), and Councillors often had the widest view of the entire picture on the ground due to all of this – which makes my point even more pedantic, because the essence of what you’re getting at is exactly right. However, I’ve noticed that sometimes conspiracy theorists/denialists/antivaxxers go for extraordinarily pedantic points as if they negate the wider argument, so I’m flagging it up for you.
Keep up the good work,
Andy Cooke
Thanks. I’ll just change it to Local Councillor. Yes, antivaxxers are sometimes pedantic. It’s a well-known strategy, to find a minor error that doesn’t change anything about the arguments, evidence or points being made and then try to use it to discredit the whole thing.
Yeah provaxxers never use sophistry ?
@johnlabarge
Thank god that you are here to present a balanced and nuanced take on the science of vaccines.
Why is “provaxxer” a thing? It’s like saying “Allopath.” These are the default states, not “Options.”
And this shows the difference beween ideologues and scientists. The latter try as hard as possible to test hypotheses. The former don’t.
@Julian: More exactly:
• The scientist works as hard as she can to prove herself wrong.
• The ideologue words as hard as he can to prove himself right.
You can tell everything about people just from how they react to correction.
More correctly, the ideologue works as hard as possible to ignore evidence that they are wrong.
“More correctly, the ideologue works as hard as possible to ignore evidence that they are wrong.”
Incorrect. For us it would require work. For them it is no effort at all.
One of the advantages of being made without a conscience.
A. Their point of the protection paradox is really interesting. If I understand correctly, they’re saying that once we figure in healthcare capacity, even with focused protection people will need to self-isolate or the healthcare system will be overwhelmed. I think they add that low-risk people likely will self-isolate if they can, once they see this.
But if people self isolate herd immunity won’t happen. So there’s a self-defeating aspect to the idea. Am I understanding correctly?
I get that for some self isolation isn’t an option, but this sound like without aggressive government effort to avoid isolation – maybe by lying about the way the virus transmits, as Sweden apparently did – this isn’t even a starter? I’m setting this out so that if I misunderstood someone can correct me.
B. The other thing this doesn’t quite capture is that the GBD’s focused protection idea comes from privilege in another way. In multiple places we have multigenerational houses. Not everyone can afford, or is culturally inclined, towards having the elderly in special care homes or alone.
Then what? How do you isolate that? Or the family with an immune compromised member?
C. The puppies are adorable. More pictures would be welcome.
The authors actually mention multigenerational households in the press release for this study. Of course, what interests me about the study is how little attention it got relative to studies that claim to find that vaccines aren’t very effective or that “lockdowns” don’t work; i.e., not very much.
“C. The puppies are adorable. More pictures would be welcome.”
QFT.
Orac writes,
“Of course, the Great Barrington Declaration was never a viable plan to deal with the pandemic.”
MJD says,
Off topic: Cute puppies, Orac.
On target: The Great Barrington Declaration could be viable in the future with a breakthrough technology that effectively inhibits cytokine storm development during acute infections.
https://ijsra.net/sites/default/files/IJSRA-2021-0196.pdf
@ Orac’s minions,
Please thoroughly read the medical paper above before commencing respectful insolence upon MJD.
That paper is great for discussion on reducing severe illness in younger people – but it doesn’t pertain to the fundamental flaws in the GBD:
1 – Unscrambling the egg: how do you segregate the entire society by age and vulnerability? We’re talking millions of people. Multigenerational households (including CV parents or over-fifties parents with children). Millions of workers over fifty, or with one or more long term conditions (by your forties, nearly 30% of adults have at least one LTC) are now totally unavailable to the workforce (including a significant proportion of healthcare workers).
Where do people live? You’re splitting millions of families up and putting them… somewhere? For how long? How many bus drivers, doctors, nurses, lorry drivers, utilities workers, etc are now unavailable? Who replaces them? How severe is the impact on the health service?
2 – How many people do you need to segregate and for how long? I cross-referred my quick-and-dirty estimate of the JVCI groups 1-9 with the Qcovid calculator and found that I’d under-played it, if anything. We’re looking at nearly 50% of the population of the UK (in order to avoid healthcare collapse – it’s IHR rather than IFR we look at here). With barely 15 million adults left to run, well, everything. Even so, the healthcare system could still collapse – partly because a big chunk of doctors and nurses are now shielding.
3 – What happens at the end? Suppose you magically unscramble the egg, and somehow manage to support them somewhere and without total collapse of everything and it runs riot through the population. You’ve now got about 50% infected – which gives herd immunity for an R0 of 2. Even Original Flavour covid had an R0 of 2.5-3, so that’s not enough – you get an outbreak in the vulnerable as soon as you release them. With Alpha, it’s up to 4.5 (so you could only isolate about 22% of the country – nowhere near enough), with Delta it’s 6-7 (you need to get 5/6ths to 6/7ths infected), and Omicron it’s 15-20+.
4 – And then reinfections screw it all up and your younger/less vulnerable people can STILL carry the chain of infections into the older/vulnerable ones, anyway, and mutations continue to erode the herd immunity wall.
So – it couldn’t be put into practice, it would have needed to isolate an absurd number of people, and the scale of those still-to-be-infected coupled with reinfections would have made it a pointless exercise even if it could have been done.
THAT’S the issue, not illness in younger people.
@MJD: “Cute puppies, Orac.”
Yeah, you really should’ve stopped while you were up, MJD. “medical paper”, LOL. Obvious rag is obvious. I could pity you for your delusions of competence were you not so indescribably boring.
@Adrian: “Unscrambling the egg … We’re talking millions of people.”
Sorry, thought you were talking about MJD’s brain. Although the confusion is understandable. Sadly you’ve more chance of extracting a chicken than a rational thought from that rancid omlette.
‘The Great Barrington Declaration could be viable in the future with a breakthrough technology’, is a great way to say that it’s not viable, without actually saying it. Why not just say it ‘GBD is nothing more than wishful thinking’? If you need a ‘breakthrough’, you are probably F**ked.
So if your analysis it right, GBD is even more of a ‘pipe-dream’ than people thought it was.
Wow, that’s a lot of pomposity in such a short comment.
Alties I read brag about how Sweden was able to do ‘so well’ with Covid despite avoiding lockdowns and other PH measures by “protecting the vulnerable” but reality based sources ( The Lancet, the Hill, Business Insider, ABC news) show otherwise: Sweden did much, much worse than the other Nordic countries.
Yet the alties persist, describing Sweden as an exemplar in pandemic response.
What’s wrong with these people? Anyone can look up the numbers.
re foster puppies! Hurrah!
during the pandemic’s early days, groups who spayed and neutered feral cats locally shut down for over a year and we were inundated with MANY outdoor cats and kittens. My SO, who fed them, later, when the shelter was functioning again, brought in several kittens for adoption, helped get a few adults spayed and found a home down the street for a 6 month old. A tiny black one, apparently without a mother, appeared in the snow, followed him around into his car and into the house, adoptinh him. So I have a brilliant black cat who plays fetch.
I’ve been reading this blog since early on in the pandemic, and as a non-medical person/non scientist, I haven’t felt qualified to comment on any posts thus far, although I’ve found the content to be most useful as a lay person to better understand the various topics covered. This comment is to thank Denise and Orac for the wonderful work they’re doing with vulnerable animals, and as the carer of four previously feral cats, I am particularly thankful to Denise and her SO for taking on the black kitten. Heartwarming story.
Sometimes they just figure out to get while the gettin’s good — I’ve had a few just appear at the back door, and my landlady, who’s out most of the night feeding feral colonies, regularly reports young ‘uns hopping into the car and
honking the hornwaiting to see where the ride goes.@ Narad:
I’m glad to see you back.
It’s amazing, there are now only 2 or 3 cats hanging around.
A local park with a wooded area beside a small river has become a feral haven.
Hi Narad. Good to see you.
As a resident of Great Barrington, I’d like to propose a simple rule that when you write about AIER and GBD, you have to say something nice about Great Barrington, lest everyone think we are this horrible town in western Massachusetts. Something like “As you drive by the despicable AIER, heading east, continue about a mile and stop by the Church made famous by Arlo Guthrie in Alice’s Restaurant”. Or “A few miles southwest of AIER, is a trailhead to the Appalachian Trail – go for a nice hike and forget all about the ‘Focused Protection’ nonsense”. On the other hand, this is where Mark Hyman started and made a name for himself and you really can’t throw a rock without hitting a reiki master or naturopath.
“you really can’t throw a rock without hitting a reiki master or naturopath”
Throw harder.
I thought Alice’s Restaurant was set in Stocksbridge, MA? Or is that just up the road?
I’d love to visit, and take twenty eight colour glossy eight by tens… etc. ?
Alice’s Restaurant is in Stockbridge, but the Church, with all the garbage that they tried to take to the dump, is in Great Barrington (technically, the village of Housatonic), but is only about a mile or so from the Stockbridge border.
Indeed the puppies are adorable and should consume your attention. More pictures please. They won’t remain puppies forever. Unfortunately Covid will be with us a lot longer.
“What’s wrong with these people? Anyone can look up the numbers.”
Altie Rule #0: Never attribute to stupidity what can adequately be explained as malice. People will choose to believe what they choose to believe. And if that belief should require feeding others into a cement mixer… well, there you go.
“A tiny black cat … followed [SO] around into his car and into the house, adopting him. So I have a brilliant black cat who plays fetch.”
Hey, take the compliment! At least some on this planet have good sense and good taste.
You’re right about the presence of malice- even when it’s inadequately disguised by feigned concern for clients’ welfare. If only there were a way to alert potential marks to warning signs. I know that Dr Barrett sketched out “signs of a bogus website”. How about signs of Lying Through Their Teeth? I’m working on it.
re the Black Cat:
she definitely found her niche. Smart, small, elegant and the first cat who doesn’t want to sleep on the computer!
re Malice:
Thinking about this, I venture that there is a way to uncover alties’ hidden motives. They INSIST that they are humanitarians and working hard to help people improve their health and lives-I even viewed 1990s videos from one of them and learned that this is nothing new-
they almost always disparage public health measures and public education.
They warn followers about how untrustworthy/ corrupt/ compromised/ wrong the government/ universities/ professionals/ corporations/ the media are. They make mind numbing blanket statements like that! There is nothing good except their guidance, individual effort, de-centralised control and entrpreneurship. Social programmes waste money and accomplish little. Public schools were great when they attended decades ago but now are sinkholes of special interests, administration and poor teaching methods.
Review what public health and education have accomplished since the days when these frauds were in school ( 1950s-1970s?) . Of course, alties and libertarians can argue that none of these changes were worthwhile but still- the mid-century period was not the paradise these dudes proclaim:
HOWEVER things were better for under educated white rural/ small town men like them. People could set themselves up as authorities with few credentials and today, having a dilapidated truck from which to sell potions has been replaced by ( sometimes) sleek, well-designed web sites with instant payment options.
“…no matter how much Kulldorff and his crew whine about being “silenced””
You can tell a lot about people by the intensity with which they clutch their pearls.
Yeah, those aren’t pearls.
My takeaway / re-statement from the above:
The GBD proposed to achieve herd immunity by isolating the most vulnerable and letting everybody else get the infection.
The majority would need to get that infection in fairly short order, so we’d get to that herd immunity threshhold and call olly olly oxenfree for the vulnerable before the “focused protection” techniques – whatever silliness they were imagined to be – lost focus and went to crapola.
This assumes everyone would go about their social interactions as normal, spreading the virus, even as the news filled with reports of severe illness. There was zero chance of that happening. Even if there was only a handful of people on ventilators at a certain point, that would have made headlines, and deep concern amongst the masses would have resulted. So people would stop going out, start shopping online, turn to Zoom for as much work as possible…
So, no herd immunity, and the pandemic goes on.
Meanwhile, the vulnerable aren’t limited to retirees and the immunocompromised, but actually include a whole lot of folks over 50 with a comorbidity or two who are still part of the workforce. People who can’t, you know, afford to not work. So the GBD actually goes beyond eugenics, as it would sacrifice a lot of “essential workers”.
Speaking of delusions, while the Brownstoners bemoan the social unrest generated by lockdowns and other mitigation measure mandates – what do they imagine would happen if either governments or even large employers had just sat on their hands, doing nothing, calling for business as usual amidst escalating sickness and death? Sure maybe the Trumpers who are screaming ‘freedom’ now would have done whatever Tucker, Trump and Joe Rogan told them to do. But they’re still only a minority, and I really doubt there wouldn’t be enough folks resisting the call to take any risk of winding up on a ventilator for the sake of the common good to cause a lot of unrest, that would itself send waves of economic consequence on down the line.
So, yeah, anybody trying to pass the GBD off as “science” has to be driven by ideology, as the ignorance of human behavior involved just can’t be explained otherwise.
This is the wrong question. The question is: Would they care?
Some men just want to watch the world burn.
Others will burn it just to rule over the ashes.
It was a rhetorical question. But the answer is, yes, they would care to a certain extent because the unrest could damage the economy. But we can both guess that the response they would advocate to such disruption wouldn’t be all that ‘libertarian’. I suppose there’s a corollary I could add to my takeaway: achieving herd immunity ‘naturally’ would not be possible* in any reasonably short term without forced compliance in getting much of the populace infected.
setting aside, just for the sake of argument, whether it would be possible at all.
“yes, they would care to a certain extent because the unrest could damage the economy”
Incorrect. They would care if it damaged their economy. But someone always gets rich from a fire sale.
From the very beginning I have characterised the GBD as impossible due to the need to care for all these people who are self isolating. All the aged care workers and their families would need to quarantine to protect the aged. Then you would need a new group of people to provide services to these people and so on. You end up with so much of the population self isolating that herd immunity becomes impossible. In the end it starts to look a lot like the Chinese full city lockdowns.
Secondly self isolating for the high risk people only works if the people around them play by the rules and avoid COVID-19 as well. As soon as one breaks the rules, COVID-19 roars through aged care homes killing indiscriminately.
Sweden basically took this approach without disaster. The mathematical modeling of the disease, from start to finish, was wrong by orders of magnitude. Hence, a mathematical analysis of the GBD’s weakness is, I’m afraid, unconvincing. China is currently proving – again – that lockdowns don’t work.
GBD in fact proposed traditional measures taken in response to all prior pandemics. Smearing its authors – all of whom had excellent medical credentials – as right-wing extremists or ignoring the second order effects on the economy – is not an argument. Thousands upon thousands of actual doctors signed the GBD. They can’t all be fringe or extremists.
I’d suggest that claims about scientists versus ideologues made in the comments reflect exactly the perspective of the GBD’s supporters against the pro-lockdown crowd.
All you’ve demonstrated is that you haven’t read Orac’s article since your false assertions are demolished therein.
I didn’t smear the authors as right wing extremists. I characterized AIER and Brownstone as right-wing propaganda astroturf houses disguised as “think tanks” and the authors, especially Martin Kulldorff, as the useful idiots that these astroturfers used.
If you’re going to attack me for being critical, at least get it right about what I actually wrote.
Do explain.
“You talkin’ to me? You talkin’ to ME?”
“I’m your Huckleberry.”
“Thousands upon thousands of actual doctors signed the GBD. They can’t all be fringe or extremists.” Argumentum ad populum fail. There are A LOT of “actual doctors” in the world. So yeah, the fringe can number in the thousands. Straw man: I said the GBD was driven by ideology, but that doesn’t make it’s supporters “extremists”, especially in the contemporary political context. That is, even ‘extreme’ free market libertarianism isn’t extremist compared to say a Big Lie Q-Anon candidate leading the race for the GOP gubanatorial primary in Michigan.
I shall leave replies to the outright falsehoods of your comment to the medical/public health pros.
Also: “Thousands upon thousands of actual doctors signed the GBD. They can’t all be fringe or extremists.”
My retort: “Back in the day, thousands upon thousands of actual doctors signed the Physicians’ Dissent from Darwinism, a creationist statement that evolution must have an “intelligent designer” and couldn’t have happened “naturally.” Back in the day, thousands of physicians signed various HIV/AIDS denialist documents claiming that AIDS isn’t caused by HIV.
Need I go on?
Argument from Authority. Argument from Incredulity. Tu quoque. Zero evidence cited. Functional illiteracy. Anything else you need to stick up your ass?
At least back in the Good Old Days the trolls here would practise foreplay before dropping their load. Quality control is obviously shot to hell. 2/10; shortest 14 seconds ever.
Glossing over your contention (“China is currently proving – again – that lockdowns don’t work.”) that Omicron, with its R0 of 15-20 or more, can’t be held back with lockdowns proves that lockdowns don’t work against original covid with it’s R0 of 2.5-3 (I’m afraid you’d have to unpack that final leap for me – especially as New Zealand and Australia are saying “wait, what?”)… and the unfounded claim about mathematical modelling (which sounds more like the Spectator, or Toby Young talking – interestingly, the famous Imperial College model now looks to have been considerably overoptimistic rather than pessimistic, but you’d not conclude that from them)…
I came in on this looking for the practicalities. If, as you say, Sweden followed this, could you clarify for me the crucial points:
1 – Where did they draw the line on which ages to give maximum shielding to, and which ages to let it run riot?
2 – Could you specify how they split up the generational families?
3 – Could you confirm that those over the age threshold (of 50? 55?) were all totally shielded (“focused protection”) and that those below the age threshold acted exactly as before?
4 – Are you claiming that this allowed all those below whatever-age-it-was to become infected and immune prior to vaccine rollout?
5 – What proportion of the country as a whole (inclusive of the older echelons) were therefore immune, and did it indeed provide herd immunity?
Because my understanding was that Sweden applied general restrictions, using recommendation rather than law (which was followed very well, as shown by mobility data), that these had a lesser maximum than their neighbouring countries (and thus the death rates went higher and came down slower than in other Scandinavian countries) but the minimum level was HIGHER than in neighbouring countries – and thus the average freedoms enjoyed were less than in neighbouring countries..
And that their death toll was a multiple of all its neighbours added together, that their response was ripped to shreds in a recent published review, and their state epidemiologist was fired. And their economic impact was actually greater than in the neighbouring comparable countries/
Oh, and their rate of bankruptcies was actually higher than here in the UK, which is pretty shocking. But possibly I’ve misunderstood?
Sweden’s approach was so successful that in December 2020 Sweden started introducing lockdown measures.
Why is it that the libertarian love of the Swedish response, but overlook how the Nordic model, including universal health care, may have contributed?
Sweden has a longer life expectancy, lower infant morality, less preventable deaths etc. than the USA, while spending a lower % of it’s GDP and less government revenue on Health care (even with a higher % of health care funding coming from the government).
So the USA spends more – and gets less.
“Thousands upon thousands of actual doctors signed the GBD.”
Millions upon millions of actual doctors (including the vast majority with applicable training and expertise) didn’t.
So your argument from popularity fails even on that basis.
Sweden actually used triage in their old people’s hom
COVID deaths were much less in Finland than in Sweden. So lockdowns do reduce deaths.
“China is currently proving – again – that lockdowns don’t work.”
Lockdowns are meant to be appropriately and judiciously applied to achieve zero or low levels of community transmission until the population is vaccinated. The failure in China – apart from the draconian measures they took to achieve lockdown – was in not getting the most vulnerable older population vaccinated. Also zero community spread became a political mantra that is being extended beyond its usefulness. It is still the mantra even now when it is obviously not possible to achieve zero community spread with the more highly infectious Omicron strain. It is certainly not what the epidemiological advice in China is advocating at present.
When appropriately and judiciously applied, lockdowns have saved countless lives.
Australia and NZ more or less applied lockdowns successfully, while the US and the UK did not. Here are the mortality rates per million for these countries:
Aus: 278
NZ: 141
US: 3,051
UK: 2,552
That is a massive difference with less economic disruption and quicker return to normal of those first two countries compared with the latter two.
@ ADM64
You write: “Sweden basically took this approach without disaster.”
Sweden had between 5 and 10 times the per capita death rate from COVID-19 as the other Scandinavian nations, Finland, Denmark, Norway, nations which did lockdown. And Sweden was among tthe highest death rates in Western Europe. Maybe your definition of “disaster” differs from mine, which considers the loss of human life that could have been prevented as a disaster.
References:
Brussalaers et al (2022 Mar 22). Evaluation of science advice during the COVID-19 pandemic in Sweden. Humanities & Social Science Communications. Available at: https://www.nature.com/articles/s41599-022-01097-5.pdf?error=cookies_not_supported&code=d7525d65-06b2-4db6-b81b-dd6d42f62e23
Barrett, Michael (2020 Dec 22). What have Norway, Finland and Denmark got right on Covid-19? Interventionist approaches to the virus in the Nordic
countries helped them avoid Sweden’s spiralling death rate. http://www.newstatesman.com
Habib, Heba (2020 Jun 12). Has Sweden’s controversial covid-19 strategy been successful? Sweden has stood out in the global pandemic by eschewing lockdown and seemingly aiming for herd immunity. Heba Habib reports that Sweden’s publicwas supportive of the strategy, but is nowpaying a heavy price. BMJ
As a retired epidemiologist who did my doctorate in Sweden, I have been both monitoring Swedish public health website and exchanging e-mails with friends. So, your claim the Swedish approach was without disaster is 180 degrees WRONG
@ Dr Joel:
Thanks for that. The loons I survey keep telling us that “Sweden was right!”.**
As Orac shows below, scoffers try to claim the same “success” for lax Florida.
Do you have any ideas about how we can present information like this to the general public in a way that misinterpretation like that about Sweden and Florida is less likely?
It seems to me that alties/ political naysayers try to find ‘soft spots’ wherein to stick their
dirty lies. How to pre-bunk, so to speak.
** another dishonest claim is citing very poor countries without much of a health infrastructure and reporting system and saying that Covid rates/ deaths were very low because the people weren’t vaccinated ( e.g. India, African nations)
So, the authors of the study conducted a “simulation,” and they used data to calibrate a few parameters. So what?
If one examines excess mortality by state (in the United States) one finds that performance over time converges. So, for example, the states of New York, California, and Florida end up performing very close to the national average with Florida performing a little better than California. All of these states clock in at about 16% excess for the whole of 2021-2021. Interesting, huh? So, it’s not obvious that there is any correlation between NPI regimes (by state) and performance by state. Simulate that. The data don’t support your heavy claim.
Actually, it’s not at all “obvious” that that is true. Confounders. Apparently you’ve never heard of them.
Quite. The simple-minded gardener’s logic lies somewhere between specious and outright baboon. I mean, IANAS and even I can figure out the numbers should NOT be converging.
The high early deaths in blue states were the product of SARS-CoV-2 rampaging unchecked through dense urban areas, decimating the vulnerable, before anyone had any clue how to treat it effectively, never mind prevent it altogether. That red states are catching up now, after more than a year of knowing how to minimize fatalities through effective treatment protocols and mass vaccination, requires absolutely concerted deliberate effort; intentionally engaging in behaviors which maximize the kill count despite all their natural advantages of distributed geography and a very late start.
Seriously, it is hard to formulate any explanation for this that doesn’t go way beyond gross incompetence to depraved indifference murder in the second degree. Although I’m sure the RI trolls will try. At any rate, not one to brag about.
The one consolation in all this is that the GOP are [hopefully] killing far more of their own voters than anyone else’s. Although GOP being GOP gone full-fascist now, their fixes are probably in already anyway so they’ve probably got idiots to spare, just as long as no-one else turns up on the day. Almost can’t wait to see what balls-to-the-wall boldness they cook up in November to ensure the ultimate victory†. Lots of early mail-in votes I would wager… some maybe 12, 18 months in advance. Ah, the benefits of carving out exceptions like coffins—Two for the Price of One!
—
† Assuming we’re all still here by then and not plate glass due to the Soviet loon going full extinction burst.
NPIs have no effect and countries end up converging?
https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-01..latest&uniformYAxis=0&pickerSort=asc&pickerMetric=location&Metric=Deaths+and+excess+mortality&Interval=7-day+rolling+average&Relative+to+Population=true&Color+by+test+positivity=false&country=USA~GBR~NZL~AUS
Looks to me like NZ and Aus will never ever come anywhere close to, say, the US and the UK in terms of either recorded cumulative death rates or (more reliably) recorded cumulative excess death rates.
Of course, there are numerous confounders, but your claim was that convergence is inevitable regardless of NPIs. Looks to be very much untrue.
Why ecess mortality in Nordic oiuntries show a diffrent result ? You take all ata intoi account.
The total death rates may have converged, but the numbers of deaths per capita after the first few months were lower in Massachusetts and New York than in states that said “we don’t need no stinking restrictions.” It’s not some kind of freaking contest, in which Minnesota or Florida was supposed to think “twice as many people have died in New York, because they had a head start, but we have time to catch up.”
There was nothing Massachusetts could do in 2021, or even in April 2020, to prevent transmission in February of 2020. There are some very smart people at MIT, but even they don’t have a time machine.
What part of SEIR models do you not understand?
No.
What data? The “interesting” factoid that you’ve barfed up isn’t going to yield dynamics, no matter how many quarters that you feed into it.
I think you mean creationists (or if you’re being tactful, cdesign proponentists) instead of evolutionists, though that actual text of “Dissent from Darwinism” takes an ultradarwinist position – it’s merely skeptical that mutation and natural selection can account for the diversity and disparity of the biota, while actual evolutionary biologists are confident that other processes operate.
I was preparing to read the article but when I read the highly opinionated initial sentence of twitter becoming more of a hellsite after the Musk purchase, I chose to read no further. I am a physician and prefer objective reviews of scientific evidence rather than opinionated pieces
Do whatever you like. I don’t care.
It does amuse me how easily triggered you appear to be, though. It was an irreverent throwaway joke that you used as an excuse to discount the entire article, which tells me all I need to know about you.
Yeah, a website called “Respectful Insolence” should not contain any snark.
Opinions are such a drag.
That’s why discerning, fact-based physicians join the AAPS.
I am getting continued amusement by people freaking out over this. One the one side, they’re all afraid he is going to “ruin” it. The place is a cesspool. On the other side, they think he’s going to bring some glorious day of twitter back. The place is, and pretty much always has been, a cesspool.
[…] for fewer interventions to slow the spread of the virus, consistent with his admiration for the Great Barrington Declaration and it’s “let COVID rip” strategy to achieve “natural herd […]
[…] Contrary to Dr. Kheriaty’s characterization, the NIH was set up the way it was in order to try to insulate it as much as was feasible against gross political manipulation (although, admittedly, it doesn’t always work, as Republicans and the a the odd Democrat have occasionally demonstrated). To sprinkle the NIH budget among 50 states would not only greatly dilute the impact of that $45 billion, but would spread it to a number of states that have indeed been nakedly political about public health and science, such as Texas or, even worse, Florida, where Gov. Ron DeSantis brought in Dr. Joseph Ladapo to run the state’s public health infrastructure. Dr. Ladapo, you might recall, was a member of the quack group America’s Frontline Doctors, which was dedicated to promoting unproven treatments like hydroxychloroquine during the summer of 2020 and then pivoted to ivermectin, promoting antivaccine misinformation about COVID-19 vaccines, and pandemic grift running a prescription mill for this similarly ineffective repurposed drug. Unsurprisingly, he is a big fan of the Great Barrington Declaration, which advocated a “let ‘er rip” approach to the pandemic in order to achieve “natural herd immunity” more rapidly. It was always an approach to the pandemic that could never have worked. […]
[…] for fewer interventions to slow the spread of the virus, consistent with his admiration for the Great Barrington Declaration and it’s “let COVID rip” strategy to achieve “natural herd […]
[…] to slow the spread of the virus, consistent with his admiration for the Great Barrington Declaration and it’s “let COVID rip” strategy to achieve “natural herd […]
[…] that 2022 is nearly halfway done, I have some questions of my own for the authors of the Great Barrington Declaration regarding the following question and answer from their […]
[…] (mostly) harmless, which is why we should just let the disease spread, the better to reach “natural herd immunity” […]
[…] is (mostly) harmless, which is why we should just let the disease spread, the better to reach “natural herd immunity” […]
[…] resisting government authority to do anything for public health and promoting a eugenicist “natural herd immunity” strategy in which COVID-19 would be allowed to rip through the “young and […]
[…] the mRNA-based COVID-19 vaccines received emergency use authorization.) It’s an approach that never would have worked, given the practical difficulties and the observation (predicted even in October 2022) that […]
[…] the mRNA-based COVID-19 vaccines received emergency use authorization.) It’s an approach that never would have worked, given the practical difficulties and the observation (predicted even in October 2022) that […]
[…] the mRNA-based COVID-19 vaccines received emergency use authorization.) It’s an approach that never would have worked, given the practical difficulties and the observation (predicted even in October 2020) that […]
[…] was clear to public health scientists, epidemiologists, and infectious disease experts that the GBD never would have worked, but since those variants demonstrated that COVID-19 evolve to overcome postinfection […]