
I’m back. My grant application is (almost) done; so by Wednesday or so I should be back to a normal blogging schedule. In the meantime, I’ve updated a discussion from elsewhere about how, every so often, there will arise a myth that can be expressed as a sound bite. The most effective ones during the pandemic are associated with a statistic or a percentage that is passed around as though it were a fact. In August 2020, for example, as the death toll from COVID-19 was skyrocketing, there arose a myth that “only 6%” of the reported deaths due to COVID-19 were actually due to COVID-19, with the rest being people who died “with COVID-19,” not “of COVID-19.” It was an utter distortion of CDC statistics at the time, but it was highly effective. Indeed, it became what I like to refer to as a “zombie stat,” a bite-sized piece of viral disinformation that, no matter how many times it’s debunked, keeps rising from the dead, although maybe I should refer to it as a “slasher” stat, because, like Jason Voorhees or Michael Myers and a host of supernatural slashers, every time it appears to be dead it always reappears in the next installation of the franchise, often in a different and more powerful form (for example, Jason didn’t even don his iconic hockey goalie mask until the third installment of Friday the 13th). Even now, early two years later, I still see this slasher statistic popping up again and again and again to kill again.
It is important to point out that slasher stats aren’t unique to the pandemic, nor are they even just restricted to conspiracy theorists and science deniers—although often that’s where they begin before finding their way into more “respectable” discourse. Before the pandemic, for example, there was the bogus statistic that medical errors are the third leading cause of death in the US, a figure that was wildly inflated in 2016 when it first really took off and, with new data since then, has become more and more detached from reality. Yet it persists and has so permeated the public discourse that it pops up everywhere as fact, including TV shows like The Resident and at the end of Peacock’s docudrama Dr. Death—even in medical news sources like STAT. Ironically, the academic most responsible for popularizing this myth in 2016 (although versions of the myth had percolated in the quack underground for years before that, such as Gary Null’s Death by Medicine) was Dr. Marty Makary, a surgical oncologist at Johns Hopkins University who has since become a leading COVID-19 minimizer, opponent of public health interventions, and general misinformation spreader, who most famously predicted in early 2021 that we’d have “herd immunity by April.” It’s over a year later now. How’d that prediction work out? Now he’s doing his damnedest to spread misinformation to frighten parents from vaccinating children against COVID-19.
A viral slasher stat from the “Pfizer data dump”?
There’s a new slasher stat in town, and I suspect that we will keep seeing it for a long time. It’s a claim that you might have been seeing all over social media that the efficacy of Pfizer’s mRNA-based vaccine BNT162b2 (now called Comirnaty) was not 95% as reported, but “only 12%”, a figure supposedly based on Pfizer’s own clinical trial documents. You can see how that would be a bombshell! An efficacy of 12% would be really weak and would not have met the FDA’s requirement for at least 50% efficacy to garner an emergency use approval (EUA). It would be serious news! It even has hashtags on Twitter now: #pfizergate, #pfizerdocuments and #pfizerdatadump, among others. Although this slasher stat seems to have appeared out of nowhere, if you’ve been paying attention you might have noticed that it actually has origins dating back nearly a year and a half from what should be—but is no longer—an unexpected place, namely a once highly respected medical journal, The BMJ.
Before I trace that origin, here are a few examples of the social media chatter, to give you an idea of how the “12%” slasher myth is playing out:
The origin of this most recent claim appears to come from the Pfizer documents currently being hosted by an antivaccine group called Public Health and Medical Professionals for Transparency (PHMPT)—the key phrase being “appears to be.” As you will see, this new slasher lie did not actually come from the Pfizer documents, but let’s follow the current claim first. Listed among the members you’ll also see some familiar names from the COVID-19 antivaccine propaganda effort (e.g., Paul Alexander, Peter McCullough, Aaron Kheriaty, and Harvey Risch) and a number of seemingly respectable academics who should know better (e.g., Peter Aaby). The website has a hilariously disingenuous disclaimer, too:
This nonprofit, made up of public health professionals, medical professionals, scientists, and journalists exists solely to obtain and disseminate the data relied upon by the FDA to license COVID-19 vaccines. The organization takes no position on the data other than that it should be made publicly available to allow independent experts to conduct their own review and analyses. Any data received will be made public on this website.
These documents come primarily from court filings based on a FOIA request for all the documents related to Pfizer’s clinical trial from PHMPT itself, which, in combination with all the COVID-19 denialists and minimizers who formed the organization, makes their claim that they “take no position on the data” disingenuous in the extreme:
The agency released 55,000 pages of COVID-19 vaccine review documents last Tuesday, following a loss in court months earlier that forced it to expedite its process to make the information available to the public. In a January court order, U.S. District Judge Mark Pittman of the Northern District of Texas required the FDA to release around 12,000 documents immediately, and then 55,000 pages a month until all documents are released — totaling more than 300,000 pages. The nonprofit that won the case, Public Health and Medical Professionals for Transparency, sued the FDA last September, claiming that the agency denied its request to expedite the release of COVID-19 vaccine review documents via the Freedom of Information Act (FOIA). In a November joint status report, the FDA proposed releasing around 500 pages of the documents each month — which would fulfill the organization’s FOIA request in about 55 to 75 years. The agency must redact confidential business and trade secret information from Pfizer and BioNTech, as well as any private information on patients in the clinical trial. In its proposal for a 55-year timeline, the FDA noted that the branch that would handle the request has only 10 employees, and is currently processing around 400 other FOIA requests.
This issue led to many antivaccine conspiracy theories claiming that ignored all the valid issues preventing the release of such a large document stash and claiming that Pfizer was going to be allowed to sit on the clinical trial data for its vaccine for 75 years. I’ll just cite one example that appeared on Robert F. Kennedy Jr.’s Children Health Defense website claiming Pfizer, FDA Hid Data Showing Clinical Trials Failed, Says Former BlackRock Advisor and Pfizer, FDA Lose Bid to Further Delay Release of COVID Vaccine Safety Data. Ironically, the latter article notes that the order required the release of:
- 10,000 pages apiece, due on or before March 1 and April 1, 2022.
- 80,000 pages apiece, to be produced on or before May 2, June 1 and July 1, 2022.
- 70,000 pages to be produced on or before Aug. 1, 2022.
- 55,000 pages per month, on or before the first business day of each month thereafter, until the release of the documents has been completed.
Per the court order, earlier this month, Pfizer released 80,000 more pages, and, unsurprisingly, COVID-19 conspiracy theorists went to work trying to cherry pick anything that they thought they could use, as predicted in the article I just cited:
“There’s a risk of cherry picking and taking things out of context,” Zalewski said. “Just because you will have all the data in front of you, that doesn’t mean you’ll reach any different conclusions.”
I expect that we’ll see more slasher stats arising and going viral in June, July, and August, and probably every month thereafter until all 300,000 pages are released, to be hosted PHMPT’s website, as antivaxxers and conspiracy theorists, who have the time go to over tens of thousands of pages of documents rapidly in order to cherry pick and take out of context various figures, do their work. Let’s just start with this one, though, since it’s everywhere.
I can’t take anywhere near sole credit for deconstructing this slasher stat alone. Dr. Jeffrey Morris and Gideon Meyerowitz-Katz have provided excellent detailed deconstructions that I draw on:
However, I will also note that the origin of a claim very similar to this is much older than the latest Pfizer “data dump.” In fact, it is a near-identical claim based on identical “reasoning” (if you can call it that) It dates back to January 2021 and appeared in The BMJ, courtesy of BMJ associate editor and antivaccine-adjacent propagandist Peter Doshi, which is when I first discussed it, as did others, such as Skeptical Raptor and John Skylar. Spoiler alert: Although Doshi came up with a figure of 19% efficacy, the latest claim of 12% efficacy is based on “reasoning” (if you can call it that) exactly like that of Doshi’s “analysis,” which is why I place a significant part of the blame on The BMJ for this latest slasher stat (I discuss Doshi in greater detail below). In fact, I go further than that. The BMJ is responsible for this claim, because it originated with one of its associate editors 16 months ago.
Let’s take a look.
A slasher myth is (re)born!
We know the claim that the Pfizer documents “really” showed that its vaccine was only 12% effective in preventing COVID-19, but it’s not as straightforward to determine when and how the claim arose after it went so viral. For this iteration of the claim, Dr. Morris and I stumbled across a post on Substack (of course!) by someone named Sonia Elijah titled “Was Pfizer’s 95% vaccine efficacy fraudulent all along?“, my having come across it in the last Tweet that I cited above. I had never heard of her before this so I thought it worth mentioning her self-description on her Substack:
I’ve written many in-depth investigative reports for TCW, Defending Freedom on: SAGE’s covert coup; the many scandals of the PCR Tests; school closures and anti-lockdown protests around the world. My ground breaking exposé uncovered the many scandals involving the Innova lateral flow test used by NHS Test & Trace, which the UK government spent £4 billion on. I also write for one of the world’s leading biomedical research sites, Trial Site News, which published my revelatory investigative series: Are the Scientific Journals Censoring the Science? My reports uncovered the major conflicts of interest, malfeasance and shocking acts of censorship, perpetrated by the scientific journals.
Trial Site News is not exactly a writing credit that I’d be proud of, given that it’s one of the biggest conspiracy sites out there and has leaned heavily into antivaccine conspiracy theories since the pandemic hit, having popped up as a culprit amplifying misinformation and conspiracy theories in a number of posts here.
The funny thing is, though, even this iteration of this piece of misinformation predates the latest Pfizer document release, as Elijah’s post is dated April 3. It can’t have originated from the 80,000 pages of documents released a couple of weeks ago. I suspect that somehow Jason Gardiner didn’t bother to look at the date of Elijah’s Substack post when he Tweeted this on May 1 (either that, or he didn’t care where the stat came from):
Unfortunately, Gardiner has nearly 143K Twitter followers, which facilitated his claim to go viral very rapidly. Even more disconnected from reality, the document on which Elijah bases her “analysis” was released to the public in December 2020 ahead of the FDA VRBAC meeting to decide on whether to issue an EUA for BNT162b2:
What Elijah appears to have done is to combine a conspiracy theory from early in the pandemic about PCR tests that led pandemic deniers and minimizers to refer to the pandemic as a “casedemic” (Indeed, Joe Mercola himself, among many others, promoted this idea.) that claimed that, because so many counts were used, the PCR test used to diagnose COVID-19 infection was producing so many false positives that weren’t actual cases of disease that in reality we were seeing a “casedemic”. As I put it at the time, “casedemic” was simply a new name for a previous COVID-19 denier trope, that increased testing explains the pandemic and that COVID-19 is not dangerous that appears to have been coined by Ivor Cummins, another COVID-19 minimizer. Personally, I’m not going to spend much time on “casedemic” given that I wrote about it nearly two years ago, and there are other contemporaneous deconstructions to which I can refer you, such as the one by Gideon Meyerowitz-Katz and Ian Mackay. I also can’t help but cite a Tweet from November 2020 to reiterate this:
But back to the 12% efficacy slasher stat and why it’s deceptive.
The “only 12% efficacy” gambit
So how did the “only 12% efficacy” gambit arise? Let’s look at Sonia Elijah’s “reasoning” (such as it is). You’ll find that it is very similar to Peter Doshi’s “reasoning” (such as it was) in early 2021, even if it arrives at a slightly different—but also low—false estimate for the efficacy of Pfizer’s vaccine. I emphasize again that her “estimate” appears to have nothing to do with the latest Pfizer release of 80K pages of documents. (If there’s something I’m missing, please point it out and I’ll add an addendum to this post.)
First, she cites the “casedemic” narrative to which she contributed, but she does it devoid of actually showing concretely how her assumption that PCR tests massively overdiagnose COVID-19, leading to a huge decline in the efficacy of the vaccine:
Firstly, it’s worth pointing out that Pfizer used a ‘central laboratory‘ (see page 13 of the document) of its choice, to confirm COVID-19 cases using a PCR test. ‘If, at any time, a participant develops acute respiratory illness, an illness visit occurs. Assessments for illness visits include a nasal (mid-turbinate) swab, which is tested at a central laboratory using a reverse transcription-polymerase chain reaction (RT-PCR) test.’ I’ve previously written an in-depth investigative report on the PCR test. The cycle threshold (CT) value used, greatly impacts the outcome of a test. According to a study by Jaafar et al., the authors found that when running PCR tests with 35 cycles or more – the accuracy dropped to 3%, meaning up to 97 % of positive results could be false positives. There is no information given on the CT value used at this ‘central laboratory.’
This claim is so divorced from reality (not to mention a total misrepresentation of the study cited) that I think I’ll just quote Meyerowitz-Katz:
Now, the author of the Substack post does not agree. They argue that, because PCR tests at high cycle thresholds do not always culture live virus, that the tests are highly unreliable and that “up to 97 % of positive results could be false positives” depending on how Pfizer ran their analysis. However, this is a very basic misunderstanding of how these tests work. The issue is that PCR tests are too accurate, rather than not accurate enough. PCR is incredibly sensitive to any viral RNA picked up, and so may identify people even if they’ve already cleared the Covid-19 infection. Indeed, the paper cited by the author of the Substack post says exactly this — if you run PCRs at a high cycle threshold, you will capture people who no longer have live virus in their body. But this isn’t a false positive by any medical definition — those with a high cycle threshold count but no live virus culture were almost always either recently infected with Covid-19 or are recuperating from an infection. In other words, they currently have Covid-19 or have very recently had the disease. It’s possible for PCRs to throw up false positives, but in most places the specificity of the test is far above 99.9%, meaning fewer than 1 in 1,000 people who don’t have Covid-19 will test positive to the disease on PCR.
I’ll also refer you to my old “casedemic” post for more detail on why this claim is nonsense, for those who are interested, as well as Dr. Morris’ excellent post, in which he notes that the only way an “analysis” (and I do use the term loosely) such as this might be appropriate is if the false positive rate is very much greater than 90%, even as he cites a PCR false positive rate of 4%, citing an FDA report for the actual PCR test used for the Pfizer clinical trial. I’ll also point out that the linking of her claims about the massive numbers of false positives from PCR tests for COVID-19 as a reason why the vaccine efficacy (VE) rate for the Pfizer vaccine was “only 12%” in its clinical trial is basically pure speculation, with no concrete evidence for her claim about PCR tests or to link her claim with the new, lower estimate she pulls out of her nether regions for the VE for the Pfizer vaccine.
In fact, if the false positive rate of the PCR test was as ridiculously high as Elijah claims, then we would not expect there to have been so many “suspected but not confirmed” cases of COVID-19 compared to actual cases that tested positive by PCR for COVID-19. Quite the contrary! We’d have expected a large percentage of those suspected cases to have been incorrectly “confirmed” by false positive PCR tests. Her linking of the “casedemic” lie about PCR tests for COVID-19 and her claim of vastly decreased vaccine efficacy compared to what Pfizer calculated are not even internally consistent! It’s true that a lot more positives would decrease the apparent VE by adding large numbers to both the numerator and denominator, thus making a smaller fractional decrease, but that’s not what appears to have happened here, given the small number of subjects with suspected COVID-19 who actually did test positive for the virus by PCR.
So let’s get to the rancid meat of Elijah’s claim:
On page 24 of the document, the results showing 95% VE (vaccine efficacy) for the vaccine can be found below.
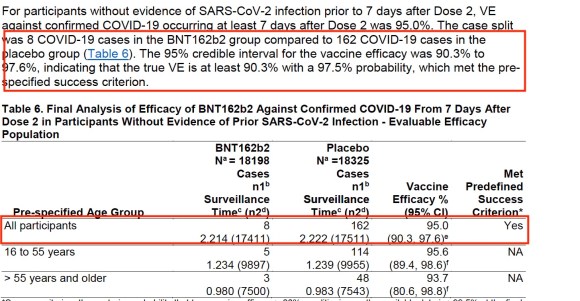
The 95% VE (vaccine efficacy) arises from the 8 confirmed Covid cases from the vaccinated group (from at least 7 days after Dose 2) compared to 162 from the placebo group. These two data points are essentially what Pfizer hang their hat on to prove their vaccine was a success! This is the data that the FDA and other regulatory bodies around the world relied upon to grant EUA (Emergency Use Authorisation) for the Pfizer-BioNTech COVID-19 vaccine and for billions of doses to be shipped around the world with some countries enforcing highly controversial draconian vaccine mandates.
A key section buried within this document, which alludes to possibly the real VE at that time, is the following damning data below (found on page 42).

These were people showing actual symptoms. If you calculate the VE from these numbers, it’s a staggeringly low 12%!
VE is calculated by dividing the difference between the case numbers in the placebo and vaccine groups, by the case number in the placebo group x 100 = VE of 12 %
It is correct that, if there were 1,594 COVID-19 cases in vaccine arm and 1,816 in placebo arm, then the VE would be 12%. However, this is not the correct calculation. For one thing, no one expected a vaccine against COVID-19 to prevent all coughs, fevers, sniffles, and other symptoms of upper respiratory viruses. Even though COVID-19 was racing through the population, there were still a lot of other upper respiratory infections going around. More importantly, as both Meyerowitz-Katz and Dr. Morris have pointed out, this calculation is based on a complete misreading of the clinical trial!
If one looks at the protocol, which is publicly accessible on the Pfizer website hosted on the FDA website, you’ll find no mention of a category of COVID-19 cases that are “suspected but unconfirmed.” There is, however, such a category listed in the FDA briefing documents, meaning that it was a description that Pfizer came up with after the trial had been run and the initial data analysis carried out. Here’s the thing. First, given that there were over 30,000 subjects it was deemed too expensive to do weekly PCR tests on all subjects; so the trial was designed to detect the ability of the vaccine to prevent symptomatic disease. That’s why the section on COVID-19 surveillance for clinical trial subjects (Section 8.13) states that subjects should contact their clinical trial site immediately and participate in an in-person or telehealth visit as soon as possible if they experience any of the following symptoms of COVID-19 (and, other than loss of sense of smell and taste, common symptoms of other respiratory viruses): fever, new or increased cough, new or increased shortness of breath, chills, new or increased muscle pain, new loss of sense of taste/smell, sore throat, diarrhea, or vomiting.
Then, the protocol dictates:
If the visit is conducted in person, obtain a nasal (midturbinate) swab (collected by site staff). Alternatively, if conducted by telehealth, instruct the participant to self-collect a nasal (midturbinate) swab and ship for assessment at the central laboratory.
In other words, the Pfizer clinical trial protocol required investigation of these suspected cases of COVID=19 to determine whether or not the symptoms being experienced by the clinical trial participants were actually due to COVID-19. Those whose PCR test was positive then became “confirmed COVID-19 cases” that were included in the primary efficacy analysis. Those whose PCR test was negative (or if done multiple times, repeatedly negative) were not COVID-19 cases. Nor should they have been counted as such!
Or, as Meyerowitz-Katz put it:
The positive tests are where we get the 8 positives and 162 negatives that the true vaccine efficacy of 95% is based on, while 3,410 tested negative on PCR and were considered “suspected but unconfirmed”. What this actually means is that these people did not have a Covid-19 infection.
Or, as Dr. Morris put it:
So these 3410 “suspected but unconfirmed” cases were people who any symptom mentioned in the list, which of course could come from many causes not just COVID-19 infections, for whom they went in for a SARS-CoV-2 PCR test, and their test result was negative. Since obviously the SARS-CoV-2 vaccine was not intended to prevent all coughs, fevers, chills, sore throats, muscle pain, shortness of breath, vomiting, etc., from any cause, it would be ridiculous to include all reports of such common symptoms as COVID-19 cases for the purpose of computing Vaccine Efficacy.
I’ll put it even more simply than either Meyerowitz-Katz or Dr. Morris put it. Trying to include these “suspected but not confirmed” cases of COVID-19 (e.g., not COVID-19) in the analysis was a transparent attempt by Sonia Elijah to dilute the effect of the vaccine by lumping in a bunch of cases that the vaccine could never have impacted in both the vaccine and placebo groups, thereby making the new “apparent” VE for the vaccine artificially low. Again, the vaccine could not and should not have been expected to prevent respiratory illnesses, but that’s what one has to expect to believe the estimate of 12% for VE. It is a claim that is just plain wrong, and it isn’t even a close call.
In fact, the only reason why someone like Elijah can make this claim seem convincing is the rather odd choice Pfizer made writing the protocol not to explicitly label as “negative” or “not having COVID-19” the suspected cases whose COVID-19 PCR test was negative. As is often the case, the least bit of ambiguity in wording can be exploited by conspiracy theorists and disinformation peddlers, and that’s what appears to have happened here.
Also:
It’s not as though Pfizer data were the only data supporting a VE of 90%, although unfortunately the rise of the Delta and Omicron variants did result in considerably lower VE.

Everything old is new again!
At this point, you might be wondering why I titled the last section “A slasher myth is (re)born“. The reason is simple. Elijah’s “analysis” isn’t even new. A version of it first appeared in January 2021, shortly after the Pfizer briefing documents had been released. It appeared, shockingly enough, in an eminent British biomedical journal, The BMJ, written by one of its associate editors Peter Doshi titled “Pfizer and Moderna’s “95% effective” vaccines—we need more details and the raw data“. Dr. Morris correctly mentions that Elijah’s “reasoning” very much resembles Doshi’s “reasoning” 16 months ago, but didn’t go into detail, preferring instead to cite his contemporaneous deconstruction of Doshi.
Let’s go back and see what Doshi wrote then:
All attention has focused on the dramatic efficacy results: Pfizer reported 170 PCR confirmed covid-19 cases, split 8 to 162 between vaccine and placebo groups. But these numbers were dwarfed by a category of disease called “suspected covid-19″—those with symptomatic covid-19 that were not PCR confirmed. According to FDA’s report on Pfizer’s vaccine, there were “3410 total cases of suspected, but unconfirmed covid-19 in the overall study population, 1594 occurred in the vaccine group vs. 1816 in the placebo group.” With 20 times more suspected than confirmed cases, this category of disease cannot be ignored simply because there was no positive PCR test result. Indeed this makes it all the more urgent to understand. A rough estimate of vaccine efficacy against developing covid-19 symptoms, with or without a positive PCR test result, would be a relative risk reduction of 19% (see footnote)—far below the 50% effectiveness threshold for authorization set by regulators. Even after removing cases occurring within 7 days of vaccination (409 on Pfizer’s vaccine vs. 287 on placebo), which should include the majority of symptoms due to short-term vaccine reactogenicity, vaccine efficacy remains low: 29% (see footnote).
Sound familiar? It should, which is why Sonia Elijah’s claim immediately sounded very familiar to me when I encountered it, given that it used basically the same “reasoning” as Doshi but came up with a slightly different estimate. Let’s compare and contrast.
Elijah used a very simple equation based on 1,594 “suspected but not confirmed” COVID-19 cases occurring in the vaccine group vs. 1,816 in the placebo group, calculating that the “true VE” should equal 1 – 1594/1816 x 100% = 0.122 or 12.2%. Note that she didn’t include the actual PCR positive cases in her calculations.
Doshi, on the other hand, did, stating that the “true” VE should equal 1 – (8+1594)/(162+1816) = 0.19 or 19%. In actuality, if indeed the “suspected” cases of COVID-19 should have been included in the calculation, Doshi actually did the calculation correctly, and Elijah screwed it up, basing her calculation solely on the “suspected but not confirmed” cases and ignoring all the confirmed cases. Both are totally wrong, though, because their calculations were based on a misreading of the clinical trial data and protocol. It’s just that Elijah was “more wrong” than Doshi and, not surprisingly, ended up with an even lower apparent VE than Doshi did. Both used exactly the same rationale, just different numbers.
Doshi also went on to answer this very criticism of his estimate in a “clarification” by likening COVID-19 to influenza and citing a Cochrane review for flu vaccines that included an analysis of their efficacy against influenza-like illnesses. In it, he used a rationale exactly the opposite of Elijah’s though. Instead of pointing to false positive PCR tests, he claimed a high false negative rate for the PCR tests. (Can these people make up their minds? Is the test generating lots of false positives or missing too much disease?) However, even according to Doshi, it would have required a huge false negative rate to have had such a dramatic impact on the calculated VE.
It’s hard not to suspect that Elijah saw Doshi’s BMJ commentary from January and decided to try to replicate it, but just botched the calculation. One might even wonder if she liked her result of 12% VE because it was lower than Doshi’s estimate of 19%.

What have we learned?
You probably wondered why I wrote early in this post that I blame The BMJ, at least in part, for the “only 12% efficacy” gambit about the Pfizer COVID-19 vaccine. It’s now a viral slasher antivaccine lie. The reason should now be apparent. The BMJ published an article that used exactly the same massively flawed rationale to downplay the efficacy of the Pfizer vaccine that antivaxxers are using now. Worse, it continues to employ the author of that commentary, Peter Doshi, as an associate editor. Doshi has used that platform to publish dubious editorials calling the safety and efficacy of not just COVID-19 vaccines, but a number of other vaccines, into question. Sixteen months ago, he published an article that made exactly the same specious argument that is now resurfaced on an antivaccine site and started spreading virally through antivaccine conspiracy social media. He just came up with a different number than Elijah did because he did the calculation right and she didn’t, but his “reasoning” was every bit as wrong as Elijah’s was. Indeed, one wonders if Elijah was inspired by Doshi’s article.
Worse, The BMJ hired Doshi despite his long history of playing footsie with the antivaccine movement since at least 2009, amplifying antivaccine conspiracy theories, downplaying the severity of influenza and thus feeding antivaccine narratives, using sleight-of-hand to downplay the effectiveness of flu vaccines, and generally playing the role of a false skeptic with respect to vaccines, as well as having signed a petition in 2006 “questioning” whether HIV causes AIDS. It continues to employ him even after he’s fallen for a conspiracy theory that the Vaccine Adverse Events Reporting System (VAERS) database was being made inaccessible to suppress report. That’s not all, though, he’s also served as an expert witness for the plaintiffs in antivaccine leader Robert F. Kennedy Jr.’s lawsuit against the University of California’s influenza vaccine mandates.
He’s only gotten worse in the COVID-19 pandemic. For example, he has used his title as a BMJ editor when taking part in a “roundtable” organized by Sen. Ron Johnson to go dumpster diving in VAERS to find “vaccine injuries” due to COVID-19 vaccines, whether the injuries were caused by them or not. In his testimony, Doshi denied that COVID-19 at the time (November 2021) was a “pandemic of the unvaccinated”, citing a report from July from the UK that most hospitalizations are among the fully vaccinated. It turned out that this report was in error, substituting “vaccinated” for “unvaccinated” and the majority of hospitalizations were among the unvaccinated, even though they made up only 31% of the population at the time. He even cited cherry-picked tables to claim that the vaccine wasn’t saving lives in what was basically an updated rehash of the nonsense he had peddled a few months earlier in which he claimed that there was “no biodistribution data” for COVID-19 vaccines and made a number of other negative false claims about the vaccines (also deconstructed by Dr. Hilda Bastian). In a truly risible moment, he even cited the Merriam-Webster definition of “antivaxxer” as opposed to those supposedly opposed to vaccine mandates to argue that he and his fellow COVID-19 contrarians were “not antivaccine” and that large numbers of people would qualify as “antivaccine”. He even parroted the antivaccine talking point that mRNA vaccines are not really vaccines and therefore shouldn’t be mandated like vaccines.
In other words, an antivax Twitter user might have come up with the clever idea of linking Pfizer’s release of 80K pages of documents a couple of weeks ago to a post from April by Sonia Elijah to imply that the “Pfizer data dump” held the previously hidden revelation that the “real VE” of Pfizer’s vaccine was really only 12% when, unless I’m missing something—and let me know if I did miss something—they contain nothing of the sort. However, the idea behind the lie that Pfizer’s own documents show that its COVID-19 vaccine is only 12% effective came from Peter Doshi, who remains employed by The BMJ despite his antivaccine activities. It is a really powerful slasher lie, too, as evidence doesn’t kill it for long. One wonders how many more times it will show up in the future. Thinking about that question, I can only think in horror of how many installments there are in the Friday the 13th, Nightmare on Elm Street, Halloween, Chucky, and Scream horror franchises.
We’re talking about many times going on for years and years and years, and we have The BMJ, at least in part, to thank for this antivaccine slasher lie that will likely never die.

21 replies on “An antivaccine slasher myth originated in The BMJ”
Against Omicron who knows. Probably less. Depending on whether we measure it as effective because someone who died was still pleased they were vaccinated whilst doing so..
There are, of course, studies:
https://onlinelibrary.wiley.com/doi/full/10.1002/jmv.27697
Booster doses are needed, because virus was allowed to spread
ERRATA: Orac wrote, “If one looks at … the FDA briefing documents.. you’ll find no mention of a category of COVID-19 cases that are ‘suspected but unconfirmed’.” However, Doshi’s quote — “3410 total cases of suspected, but unconfirmed covid-19 in the overall study population, 1594 occurred in the vaccine group vs. 1816 in the placebo group.” Does come directly from the FDA report, in a section subtitled “Suspected COVID-19 Cases” on p. 42, where the terminology is also employed 3 other times.
OK, with that out of the way… This whole meme seems to come down to Doshi either misunderstanding or misrepresenting the meaning of that phrase “suspected but unconfirmed”. I might suspect that he was combing through the document looking for something he could use as a “Gotcha!” by taking it out of context, but I can’t parse the overall context of the document well enough to confirm that… ;- \
I’m may not be qualified to pass judgement on matters of medical science, but I feel safe opining on ethical standards in journalism. I can also testify that few in the media would claim their truth standards are or ought to be as rigorous as those of medical science. Yet, any legitimate news organization (e.g. not Murdochian) would not let an error as egregious as that 19% miscalculation stand without some sort of mea culpa.
As I understand it, Doshi’s position at BMJ falls under the rubric of “commentary”, which in journo terms offers more leeway for fudging than “news reporting” (e.g. ‘opinion’ pieces get away with misleading use of true data all the time). [I shall leave aside discussion that ‘commentary’ may be a problematic function for a medical science journal.} However, even editorialists have a certain obligation to avoid outright material falsehoods. If Doshi does in fact have a history of making repeated “negative false claims about…” anything a credible media outlet would indeed fire him.
Actually, it is true that there is no category of “suspected but unconfirmed” cases in the actual clinical trial protocol, which is what I meant. (I see what you did with that ellipsis there.)
Ellipsis or no ellipsis, I will concede that the I would have been more clear and specified the category in the briefing documents; so I’ve fixed the paragraph. That was just careless of me.
As for The BMJ and its commitment to journalistic ethics, its editors have already demonstrated a distinct lack of attention to ethics, given that they haven’t corrected any of Doshi’s numerous misstatements and they keep publishing Paul Thacker’s hit pieces.
FWIW, I assumed it was an editing error, as I don’t imagine you’d fail to recognize the direct quote from Doshi.
I do think the clarity is important though, in that I think it matters that Doshi has grasped onto a phrase from an actual quote he can mis-represent, rather than make sup his own term out of whole cloth. I mean, it’s either more devious, or more irresponsible, depending.
Another thing I thought about the canon of journo ethics, but didn’t include before – in a piece like this, if there’s any doubt about what a quote means, the journalist has a responsibility to check back with the source and get clarification before publishing. I would consider Doshi should have recognized that phrase didn’t mean what he presented it as from the context — which is not about vaccine efficiency at all, but an explanation of why the data do not support concerns that the research design “could have masked clinically significant adverse events.”
To be honest, Doshi seems to function more like a glorified blogger than a journalist. Don’t get me wrong. I’m a blogger; I don’t mean to disparage bloggers. However, we are not journalists. In my case, I tend just to comment on what is publicly available knowledge and commentary; it’s not as though I contact RFK Jr. when I do a post taking down a piece of propaganda he’s promoting. Maybe another way to think of Doshi is as a cable news channel pundit or an op-ed writer in a newspaper.
That being said, The BMJ really needs to hold its editors to a higher standard, even when they are functioning more or less as glorified bloggers or pundits.
@ Orac:
” it’s not as though I contact RFK jr when I do a post taking down a piece of propaganda he’s promoting..”
BUT I wish you would!
It seems that the graf still needs a touchup for “publicly accessible on the Pfizer website hosted on the FDA website”
Vaccines being “only 12% effective” fits in with a larger vaccine/ SBM denialist myth:
vaccines don’t really work and neither do most meds with chemotherapy at “3%” efficacy ( as SBM is the third – or these days, the greatest killer with a million deaths a year- see PRN).
Which fits into the worldview that the cult of the professional misleads the public into believing that professionals know more and are more effective than average people ( see anti-vax mother warriors, altie woo, reddit, NN, Del et al).
A couple of weeks ago Bill Maher and a female former sportscaster/ present day political advisor agreed that university is quite useless: ” I didn’t learn anything”, he admitted.
Maybe it was… for them but they managed to get themselves high paying media careers. What would Maher have done otherwise as high school grad in NJ? Work in a mall?
I think that alties who cosplay professionals/ knowledgeable adults DO know at heart that they aren’t truly different from the average and maintain the same prejudices and lack of awareness of reality which enable them to truly understand and identify with their audience.
He’s a crank but he has a (misguided) point. I can’t see the value of a kid taking out $200k+ in debt to graduate with a BA in radical art theory with zero chance of getting a job or paying that back. Same kid is far better off learning a trade.
When I had the misfortune of being a TA (Required for masters and doctorate both, which sucked) I ran across more than a few students in a brick-and-mortar university setting, in the sciences who were functionally-illiterate.
Being there was doing them no good. Even if they graduated, they couldn’t understand basic scientific concepts let alone the deeper meaning attached. It was all about checking a box that said they took a science course. I’m sure the same goes for the humanities.
Don’t get me started on the three “Athletes” we had in one of our sections and what they got away with.
They really have turned into worthless-degree factories and I’m ashamed to have participated in it. That’s just my $0.02
@ Dr Yeti:
I partially agree with you that MANY people waste lots of their parents’ or loaned money acquiring degrees that don’t help them enter a career and pay their debt BUT
there are other pathways to formal education that provide meaningful skills.
— Maher is an interesting example: he went to Cornell IIRC and has made a shitload of money as a comedian/ writer/ producer. Could he have done that without a degree? I don’t know. His guest also made money as a sports reporter and political advisor- hardly high school level skills.
It should be noted that Maher, even with his degree, still gets vaccines and general health concepts wrong as Orac has noted many times. Basic science is often lacking even at elite schools.
— I would argue that a university education gives kids entrance to the world outside their day-to-day experiences in their own social group with increased diversity and small amounts of study in many disciplines so that they understand the world a bit better and at least be able to comprehend what’s happening in the news.
I think that this is particularly meaningful for women ( and perhaps minorities) to gain a sense of agency being out in the world competing against all types of people in multiple realms. I don’t imagine that expensive private schools are the only way.
While I did attend those “elitist” enclaves/ international study- without debt-most of the students I’ve advised seek out reasonably priced alternatives and less esoteric majors. Trades aren’t the only answer: technology and other skilled areas can be.
I think that I am truly different than I was when I started university: it gave me an outlook based upon more systematic and abstract perspectives rather than immediate reaction to what I encounter. And I don’t come from disadvantage : my parents and grandparents were all business people with assets. I imagine that university experience might be even more important to more disadvantaged people.
Fair enough
This emphasis on the symptom rather than the virus causing the illness is somewhat like the switch pulled about the polio vaccines.
Health workers looking for polio outbreaks watched for multiple cases of acute flaccid myelitis. They would then test the patients for poliomyelitis and do ring vaccination. This gave more attention to cases of AFM. But it also gave a tiny background for antivaxxers who would often claim that the vaccines hadn’t eradicated polio, it had just been relabeled as AFM.
AoA has been riding that mule for over a decade. EV-D68 really got them riled, in part because “they want to blame [AFM] on a virus,” etc.
I haven’t seen it documented on RI, but we have lost one of the titans of the antivaccination movement, Bill Sardi. I suspected something was up due to the latest articles on Resveratrol News being from January.
According to the following article, Bill did NOT have Covid-19 (despite a positive test), was treated with a bunch of things including ivermectin and high-dose intravenous vitamin C, but was laid low by Fauci treatment protocols and the hospital’s insistence on care approved by a power of attorney instead of relying on Bill’s allies in the Robert Schuller Ministries, Frontline Doctors etc. There is also speculation about what was really up with Bill’s Mysterious Medical Disorder* and even the possibility of poisoning, which as you will recall, did in pioneering healer Royal Rife.
https://hbnshow.com/we-lost-bill-sardi/
R.I.P, Bill.
*it is indeed mysterious that with all the resveratrol he took, Bill did not live well past 100. We should remember Bill’s teachings about Covid-19 (“Don’t Panic”, he posted last August) and continue avoiding those “vaccines”.
Perhaps we might explain it like this: There were a few thousand people who got a cold during the trials. When checked for Covid, they turned out not to have it. Now, the anti-vaccine people are pretending that they must have had Covid, and this is what allows them to do their fake calculations. It’s curious that these same anti-vaccine people are simultaneously claiming that Covid is rare — a hoax even — which would certainly go against the idea that those thousands of people had Covid, that rare disease which is a hoax.
[…] In fact, he was worse than wrong. Doshi’s methodology turned into an antivaccine meme that still circulates today, albeit in a slightly different form. It’s a technique that he’s used to attack […]
[…] H1N1 pandemic in 2009. Indeed, one of his “reanalyses” resulted in what I like to call the “slasher lie” about the Pfizer vaccine that it is only 12-19% effective against […]
[…] why the FDA estimated that it would take from 55-75 years to release all the requested documents is not due to nefarious intent, but rather because of the sheer mass of documents requested (which require redaction of […]
[…] is not to claim that it doesn’t prevent severe disease (although, to be sure, antivaxxers do that a lot too) but to call into question the legitimacy of its approval by the UK and EUA in the US, in […]
[…] why the FDA estimated that it would take from 55-75 years to release all the requested documents is not due to nefarious intent, but rather because of the sheer mass of documents requested (which require redaction of […]